Today’s dentists face a complex patient population. Aging, comorbidities and advances in evidence-based practice provide expansive and ever-changing best practice guidelines for every level of dental care. Real life scenarios create an environment in which dental practitioners must practice intelligently and defensively. The ability to conduct an accurate patient risk evaluation becomes the basis for informed practice, patient selection and risk mitigation. The goal of this article is to review dental patient risk evaluation to promote dental patient safety by considering the widely used ASA Physical Classification (ASAPC) guidelines and its application to the dental patient.
One of the most common risk assessments in dental practice is the American Association of ASA (Figure 1). Few may realize that the ASA Physical Classification system evolved from the field of dentistry. The ASAPC was developed almost 20 years after the first risk assessment classifications of dental patients. The early dental classification systems were proposed in the 1940’s. The first proposed classification system was offered by dentist turned anesthesiologist, Leonard Monheim. Leonard Monheim’s system offered a basic “A,B or C” classification. During the same decade, oral surgeon, W. Harry Archer, developed a second patient classification system. Dr. Archer’s classification proposed a “1,2 or 3” patient classification system. The proposed systems were later developed into the ASAPC The classification system is still widely used today in medicine and provides the foundation for dental patient risk evaluation.
In 1963, the ASA published it’s first version of the patient physical classification system. The classification system was developed to assess patient risks for patients undergoing sedation/anesthesia. The original publication consisted of 5 categories. A sixth category was later added. Each category is commonly referred to as “ASA Class “. A number one through six is assigned to describe patient characteristics. Stating the classification number infers that the dental practitioner is familiar with the patient characteristics in each classification. Additionally, the American Dental Association (ADA) guidelines imply dental professionals have a working knowledge of this system in order to safely select patients for the appropriate level of dental practice. Such inferences warrant a review of the ASA Physical Status guidelines and their application to dentistry.
Figure 1
- ASA 1: A normal healthy patient. Example: Fit, nonobese (BMI under 30), a nonsmoking patient with good exercise tolerance.
- ASA 2: A patient with a mild systemic disease. Example: Patient with no functional limitations and a well-controlled disease (e.g., treated hypertension, obesity with BMI under 35, frequent social drinker or is a cigarette smoker).
- ASA 3: A patient with a severe systemic disease that is not life-threatening. Example: Patient with some functional limitation as a result of disease (e.g., poorly treated hypertension or diabetes, morbid obesity, chronic renal failure, a bronchospastic disease with intermittent exacerbation, stable angina, implanted pacemaker).
- ASA 4: A patient with a severe systemic disease that is a constant threat to life. Example: Patient with functional limitation from severe, life-threatening disease (e.g., unstable angina, poorly controlled COPD, symptomatic CHF, recent (less than three months ago) myocardial infarction or stroke.
- ASA 5: A moribund patient who is not expected to survive without the operation. The patient is not expected to survive beyond the next 24 hours without surgery. Examples: ruptured abdominal aortic aneurysm, massive trauma, and extensive intracranial hemorrhage with mass effect.
- ASA 6: A brain-dead patient whose organs are being removed with the intention of transplanting them into another patient.
Adapted from https://https:www.asahq.org/resources/clinical-information/asa-physical-status-classification-system.
The ASAPC System in dentistry
In 1979, Malamed and McCarthy published an article and dental school manual to adjust the ASAPC system to meet the needs of the dental patient. They eliminated the ASA classifications of V and above. Multiple literature sources incorporate the evaluation of patient anxiety into dental patient classification. Additionally, the ADA incorporated more examples into its publications to allow a better understanding of co-morbidities to assist the dentist to more actively evaluate the dental patient’s risk for undertaking dental procedures.
ASA Physical Classification System from Dental Literature
|
ASA I
|
Little or no anxiety
|
|
|
No changes from ASAPC system
|
|
ASA II
|
Less stress tolerant.
|
|
|
Moderate to extreme fear of dentistry.
|
|
|
No changes from ASAPC system.
|
|
ASA III
|
Additional information to clarify the ASAPC system
|
|
|
Substantive functional limitations
|
|
|
One or more moderate to severe diseases:
Poorly controlled diabetes
Poorly controlled hypertension
Morbid obesity (BMI >40)
Alcohol dependence or abuse
Implanted Pacemaker
Moderate reduction of Ejection Fraction
End-Stage renal disease undergoing routine dialysis
History of the following in prior 3-12month period:
Myocardial Infarction
Coronary artery disease with stents.
Cerebrovascular accident. (CVA)
Trans-ischemic attack (TIA)
|
|
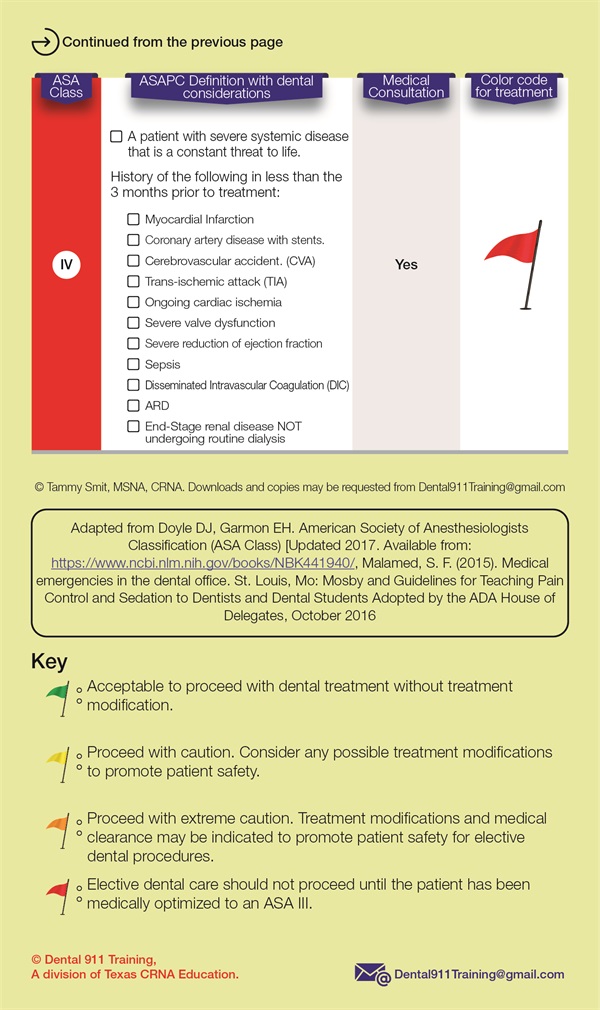
ASA IV
|
Additional information to clarify the ASAPC system
|
|
|
History of the following in less than the 3 months prior to treatment:
Myocardial Infarction
Coronary artery disease with stents.
Cerebrovascular accident. (CVA)
Trans-ischemic attack (TIA)
Ongoing cardiac ischemia
Severe valve dysfunction
Severe reduction of ejection fraction
Sepsis
Disseminated Intravascular Coagulation (DIC)
ARD
End-Stage renal disease NOT undergoing routine dialysis
|
Adapted from Doyle DJ, Garmon EH. American Society of Anesthesiologists Classification (ASA Class) [Updated 2017 Oct 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441940/, Malamed, S. F. (2015). Medical emergencies in the dental office. St. Louis, Mo: Mosby and Guidelines for Teaching Pain Control and Sedation to Dentists and Dental Students Adopted by the ADA House of Delegates, October 2016
Since 1979 there have been little to no changes in the ASAPC system in dentistry. It is increasingly difficult to ascertain what patient characteristics can be treated throughout all levels of dentistry. We are currently working on a continuing education module that assists dentists in defining ambiguous terms used in the ASAPC system in dentistry such as "well-controlled" and "function capacity/limitations". A result of our literature search has resulted in a proposed ASAPC system that incorporates both medicine and dentistry. The ASAPC system with dental considerations contains criteria from both medicine and dentistry with a checklist that is easy to use in everyday dentistry. For a copy of this checklist please email Dental911Training@gmail.com
ASA Physical Classification with Dental Considerations
© Tammy Smit, MSNA, CRNA of Dental911Training.com