Left unrestored, a single missing tooth sets off a chain of structural problems. Adjacent teeth migrate toward the vacant space, occlusion deteriorates, and the alveolar bone, deprived of root stimulation, begins a slow resorption that no toothbrush or rinse will arrest. Choosing a tooth replacement option requires consideration of both short-term treatment goals and long-term oral health outcomes. Modern dentistry offers two principal restorations: the implant and the bridge. The dental bridge vs implant comparison below examines cost, treatment duration, biological impact, and durability, the four variables that decide most cases.
What Are Dental Implants and Dental Bridges?
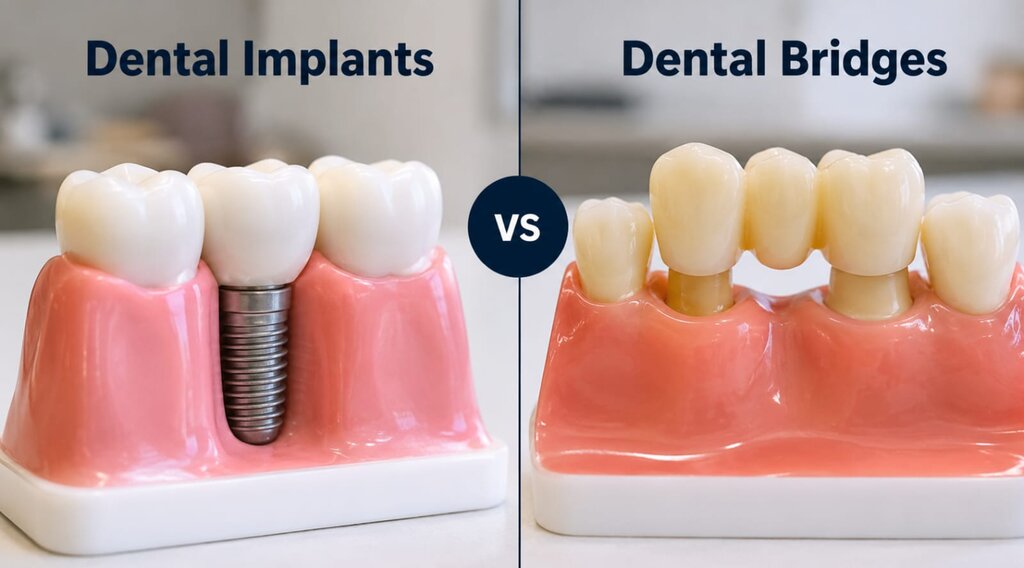
An implant replaces the root itself. A titanium post is placed in the jaw under local anesthesia; over the next three to nine months, bone fuses to its surface through a process called osseointegration, after which an abutment and crown complete the restoration. The finished tooth carries chewing force the way a natural tooth does, through the bone rather than across it.
A bridge, by contrast, spans the gap without entering it. The simplest description of what a bridge is would be an artificial tooth, the pontic, held between two anchors. Of the available bridges teeth replacement designs, three dominate clinical practice. The traditional fixed version cements crowns over the two teeth flanking the gap. The Maryland type bonds metal or ceramic wings to the lingual surfaces of those teeth, sacrificing strength for conservatism. Where several consecutive teeth are missing, an implant-supported bridge, anchored to posts rather than to natural teeth, becomes the design of choice.
The primary difference between implants and bridges lies in how the restoration is supported. Dental implants are supported directly by the jawbone, while traditional bridges rely on adjacent teeth. That difference explains the gaps in cost, lifespan, and long-term effects described below. Dentists generally favor the implant when a single gap sits between healthy teeth and enough bone, and the bridge when those teeth already need crowns, when surgery is not advisable, or when time is limited.
Cost, Treatment Time, and Recovery Differences
Any candid discussion of bridge vs implant costs begins with the published figures. A complete single implant, post, abutment, and crown together, runs $3,000 to $5,000 in current US practice. Traditional three-unit bridges occupy a $2,000 to $5,000 band; the Maryland design costs less, roughly $1,500 to $2,500. Quotes deserve scrutiny, since ancillary procedures, bone grafting in particular, and sinus augmentation where the posterior maxilla is involved, can add four figures to an implant estimate. Insurance reimbursement follows its own logic: bridges are routinely covered as standard prosthodontics, whereas implant surgery is still classified by many plans as elective.
The timelines diverge even more sharply than the prices. Two appointments over two to three weeks usually suffice for a bridge. An implant cannot be hurried, because the crown waits on osseointegration, and the full sequence takes three to nine months. Postsurgical implant recovery time itself is brief, a matter of days, followed by roughly a week of soft diet. No comparable healing period attaches to a bridge.
Considered across twenty years rather than one, the fixed bridge vs implants calculation often reverses. A bridge replaced at the typical five-to-fifteen-year interval may be purchased twice or three times within the working life of a single implant, eroding its initial price advantage.
Long-Term Impact on Your Teeth and Jawbone
Nowhere do the bridge vs implant pros and cons separate more decisively than in their biological cost. Seating a traditional bridge obliges the dentist to reduce two healthy teeth to receive crowns. Enamel removed in that preparation is gone permanently, and the prepared abutments thereafter carry the occlusal load of three teeth. Decay beneath a crown margin, a known weak point, frequently ends a bridge's service life.
The implant imposes no such tax on its neighbors, and it answers a problem the bridge leaves untouched: resorption. Once a root is lost, the bone that held it loses its functional stimulus; published measurements show the ridge surrendering a substantial fraction of its width within six months of extraction. By loading the bone directly, an implant supplies the stimulus a root once provided, preserving both ridge volume and, over time, facial contour. Beneath the pontic of a bridge, the bone simply continues to recede.
Daily Comfort, Maintenance, and Durability
Functionally, both restorations return the patient to unremarkable eating and speech, which is the point of treatment. Anchored in bone, the implant most nearly reproduces natural proprioception, and its hygiene regimen is ordinary brushing and flossing. The bridge demands one additional habit: the undersurface of the pontic must be cleaned with a floss threader or water flosser, because plaque accumulating there attacks the very abutment teeth on which the restoration depends.
On the question of how long do dental implants last, the literature is unusually consistent. A 2019 meta-analysis placed ten-year implant survival at 96 percent; fixtures surviving that interval commonly serve for decades, though crowns may be remade along the way. Bridge longevity is shorter and more variable, five to fifteen years in most series, with hygiene and design accounting for much of the spread. Regular professional review extends the service life of either restoration.
Which Option Is Right for You?
No general rule settles the question of which is better dental implants or bridges question, because the deciding factors, bone volume, gum health, overall health, budget, and patience for a months-long process, differ from patient to patient. Where health and bone allow, the implant is usually the sounder long-term investment: neighboring teeth remain untouched and the bone keeps its stimulation. The bridge or implant tooth decision tilts toward the bridge when funds are limited, when surgery carries added risk, or when the restoration must be completed quickly.
Certain findings shift the recommendation. Heavy smoking, uncontrolled diabetes, and deficient bone all compromise implant healing; conversely, abutment teeth already destined for crowns argue for a bridge, since the required preparation then serves double duty. None of this can be settled from an article. Examination, imaging, and a medical history review come first, and a detailed discussion of Dental Implants with a qualified provider settles whether the surgical route fits the individual case.